
How To Get (And Keep!) Your Knees Healthy for a Lifetime
Today we’re going to cover the basics of knee pain – whether you’re an end-user, a trainer/coach, or somewhere in between, I hope this piece gives you an understanding of my core philosophy behind long-term knee health.
Rule #1 – Do No Harm!
Are we seeing a trend here?
In my shoulder and low back series’ (available in my newsletter archives), this was one of my prevailing thoughts. If you don’t know what to do when someone is injured, the very least you can do is keep them out of pain by restricting their activities and playing it smart.
Obviously, this isn’t the ideal situation – but it’s a thousand times better than making things worse!
Rule #2 – Get a Quality Diagnosis
Write this one down: Knee pain rarely stems from a solely knee-based issue.
One of the issues that continue to plague our industry (and as an “industry,” I’m talking everyone from PT’s to trainers, coaches to orthos, etc.) is that people fail to recognize the body works as a functional unit.
If someone enters your facility with knee pain, you just check out his or her knees. Right?

WRONG!
I’m all for a “knee” assessment at the start. Dr. Shelbourne (one of the foremost experts on ACL surgery and rehab) begins every single knee assessment he does by examining knee extension and knee flexion range of motion. If knee flexion and extension aren’t symmetrical between sides, these are the first things to get addressed in their training.
More importantly, he has evidence-based results to back him up. So again, I’m not saying NOT to examine the joint in question.
However, there are tons of analogies out there – some will say the knee is a dumb joint, others will say it’s a slave to the ankles and hips. Both aren’t too far from the truth; the knee only has so much say in its own fate.
And therefore, a knee only assessment can only provide you with so much information.
When you’re training someone with knee pain of any sort, it’s very rare that the knee pain is solely a knee issue. There are obviously times when a structure in the knee is causing pain (torn ACL, menisci, etc., severe arthritic changes, etc.) but even some seemingly “knee” based issues such as patellar tendinosis are manifested due to bigger issues throughout the kinetic chain.
Here’s a practical example: I had a client come down from Chicago two years ago who had suffered from “patellar tendonitis” (aka jumpers knee) for the past 4 years. His sports med professional up there gave the diagnosis of tendonitis to him, and it had plagued him like no other. The ONLY thing these people had examined was his knee, and his rehab protocol consisted of ice, rest, and possibly some modalities.
He was a very athletic guy who was playing both volleyball and basketball at the time, so you can imagine how a painful knee condition like this had been holding back his performance.
We started examining him, and it was no wonder this guy had knee pain. Horribly short hip flexors, a significant shift on his squatting pattern, and a host of other issues left me with no other conclusion: He was suffering from patellar tendinosis, not patellar tendonitis.
Here is a quick list of what we did to get him fixed up:
- Performed an eccentric single-leg squat protocol on a decline slant board twice per day to encourage tendon strength and development.
- Worked diligently to loosen up his flexors via soft-tissue work, static stretching, dynamic stretching, single-leg training, etc.
- Strengthened his posterior chain, and really hammered his hip stabilizers.
- Made him conscious of his shift on bilateral movements so that he could correct it.
Within two months he was playing volleyball virtually pain-free, even during long weekend tournaments where he would play up to 10 matches over the course of 3-4 days.

Bottom line? If you want to develop a holistic approach to knee health, you need to assess a number of different areas: Hip and ankle mobility, tissue quality of the surrounding areas (gastroc, hamstrings, quads, TFL/IT Band, and a host of other structures too numerous to note here), foot stability, hip stability, etc.
Quite simply, looking solely at someone’s knee is a sure-fire way to miss some potentially huge pieces of the puzzle. Make sure your assessment is on point and looks beyond the joint in question.
Rule #3 – Figure Out What Hurts
While this may fly in the face to point #1, it needs to be said: Beyond just doing no harm, you need to figure out what exactly hurts and avoid that motion, at least in the short-term.
With the lower back, if some rounds their lumbar spine and gets pain, they’re flexion intolerant. You keep them out of flexion.
The opposite is true as well – if they have pain with lumbar extension, you keep them out of extension.
Here’s a knee example: We had a guy come into our gym a few months ago who had 70% of his lateral meniscus removed. Conventional wisdom would say, “Don’t squat this guy.”
However, when Bill took him through his assessment, this guy could actually squat below parallel 100% pain-free! We could argue whether heavy squatting was a good thing for him from a long-term perspective, but I simply use this to make a point.
We can’t assume what should or shouldn’t work. Some people may come to us with horrible MRI’s or X-ray’s, yet they are wonderfully functional and pain-free.
In contrast, others may have the cleanest radiology reports known to man, yet every subtle movement causes them pain.
Everyone is individual. Figure out what works (and what doesn’t) and then prescribe and coach exercises accordingly.
Rule #4 – Hammer those hips!
While the knee may be a dumb joint, the hip actually has a lot of “say” in what goes on that the knee with regards to its position, alignment, etc..
Some of the strongest evidence we have in regard to the link between knee pain and hip dysfunction comes in the form of research on patello-femoral pain. For years, people stated that patello-femoral pain was due to an imbalance between the quadriceps.
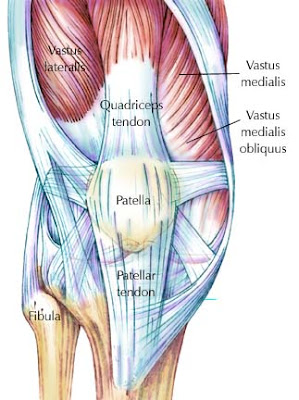
Here’s the theory: If you can imagine a tug-of-war going on at the knee, the vastus lateralis (your outer quad muscle) is stronger/stiffer than the vastus medialis obliquus (your inner quad muscle). As a result, this lateral pull causes irritation on the outer portion of your knee joint.
In recent years, there’s been a plethora of evidence mounting in support of hip dysfunction being directly correlated to patello-femoral pain [1-4]. If you have weak or unstable hips, chances are it could manifest itself in knee pain.
This is where a balance of low-level, motor control type exercises and bigger lifts come into play. Even though some people are quick to pooh-pooh isolation exercises such as glute bridges, clam shells, etc., they serve a purpose. Many clients and athletes are terribly dysfunctional, so it doesn’t hurt to dedicate some training time to teaching people how to utilize these underdeveloped or under-recruited muscle groups.
The battle doesn’t end there, though. This is one of the biggest drawbacks of “corrective exercise” – it doesn’t stop with the isolative exercises! Once you figure out what’s weak you isolate it out to improve recruitment and motor control, but you have to take that new-found strength/stability and build it back into actual movement patterns like squats, deadlifts, single-leg work, etc.
I didn’t mention the pelvis here much, but that’s only because I have bigger things in mind for that joint. If you want a primer, feel free to check out Muscle Imbalances Revealed, where I outlined my exact approach to training the pelvis and hips. Needless to say, forgetting about the pelvis is a huge no-no – if you can’t control your pelvis, your hips aren’t going to be in the right position.
Summary
I hope you have a better idea as to my basic philosophy on knee pain, as well as ways to start addressing it. Whether you’re a trainer, coach, or end-user, knowing more about the human body is never a bad thing.
In Part II of this series, we’ll discuss the actual training interventions I use to get someone healthy and back in action.
Stay strong
MR
References
1. Ireland, M.L., et al., Hip strength in females with and without patellofemoral pain. J Orthop Sports Phys Ther, 2003. 33(11): p. 671-6.
2. Prins, M.R. and P. van der Wurff, Females with patellofemoral pain syndrome have weak hip muscles: a systematic review. Aust J Physiother, 2009. 55(1): p. 9-15.
3. Long-Rossi, F. and G.B. Salsich, Pain and hip lateral rotator muscle strength contribute to functional status in females with patellofemoral pain. Physiother Res Int, 2010. 15(1): p. 57-64.
4. Powers, C.M., The influence of altered lower-extremity kinematics on patellofemoral joint dysfunction: a theoretical perspective. J Orthop Sports Phys Ther, 2003. 33(11): p. 639-46.